
INFORMATIE
English pagesSchrijf ons
Links
Disclaimer
WIST U DAT ?
BroodfokkersDermacentor teek
Euthanasie
Reverse Sneezing
De tweedehands hond
Zonnesteek
HISTIOCYTOSE
Histiocytaire TumorenHistiocytose bij honden
Histio Lotgenoten
Vragenlijst (download)
Onderzoeksrapport
Histio Forum
IMMUUNSYSTEEM
Auto-immuunziektesSHELTIES
CorkyPhoebe
Stambomen
Regenboogbrug
Foto en video archief


Histiocytaire neoplasiën en verschijningsvormen
Dr. Paul J.J. Mandigers
Dierenarts-specialist Interne Geneeskunde
***
Veterinair
Specialistisch Centrum "De Wagenrenk"
Keijenbergseweg 18
6705 BN Wageningen

Inleiding
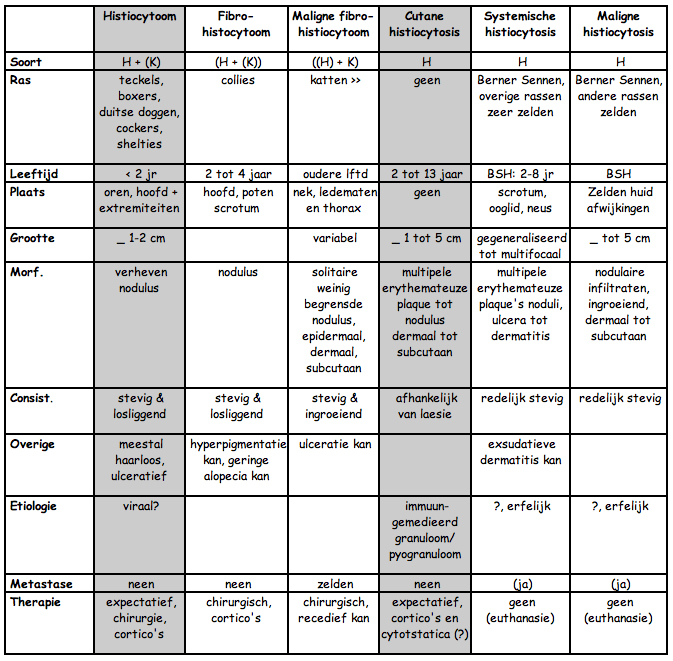
Er is veel discussie over histiocytaire tumoren. De reden is dat veel oudere publicaties gebaseerd zijn op alleen kern-morfologie en/of andere eigenschappen van histiocyten (fagocytose). De laatste jaren worden ook andere detectie methoden (electronenmicroscopie) en speciale kleuringstechnieken (immuun-histiochemisch, etc) gebruikt. Niet altijd is dan ook meer duidelijk wat voor een soort neoplasia men beschrijft. Want met het gebruik van nieuwe technieken veranderen niet alleen namen maar ook worden sommige tumoren buiten de groep geplaatst (bijv. a-typische histiocytomen) en andere juist ingesloten (sommige fibrosarcomen). Daarnaast wensen sommige auteurs te spreken van fibro-histiocytaire tumoren. Dit door het gemengde celtype van fibro- en maligne fibro- histiocytomen (4). Voor dit praatje wordt gehanteerd de indeling volgens Muller et al., (5). Deze indeling is echter niet geheel actueel meer. Maar voor de eenvoud wel te prefereren. Hierbij worden de tumoren in histiocytomen en histiocytosis ingedeeld. Een onlangs verschenen werk (4) tornt nogal aan de indeling en naamgeving. De indeling van Muller et al., (5) is:
| - | Histiocytomen |
| * histiocytomen | |
| * fibro-histiocytomen | |
| * maligne fibro-histiocytomen | |
| - | Histiocytose |
| * cutane histiocytose | |
| * maligne histiocytose | |
| * systemische histiocytose |
Achtereenvolgens worden de tumoren beschreven en waar van toepassing de indeling bediscussieerd. Naast de zes typen van histiocytaire neoplasiën komen er nog diverse andere neoplasiën voor die eerst wel en/of niet histiocytair genoemd werden. Voorbeelden zijn de Merkel-cel tumor (a-typische histiocytoom), Sticker tumor (venerisch overdraagbaar condyloom). Omdat deze niet langer genoemd worden onder het hoofdstuk histiocytaire verschijningsvormen worden deze ook hier niet genoemd. De tumor a-typisch histiocytoom is ten onrechte een histiocytoom genoemd. Hij wordt heden ten dage beschreven onder de naam muco-cutaan extramedullair plasmacytoom (4). Hij zal niet verder besproken worden.

GEHANTEERDE DEFINITIES:
Histiocyt:
Een histiocyt is een grote fagocyterende interstitiële cel,
onderdeel van het mono-nucleaire fagocyten systeem. Het is een
macrophaag (1). Het cytoplasma kleurt eenkleurig of eosinofiel
aan. Ze hebben een grote gekorrelde kern met een duidelijk kernlichaampje
(3). Feitelijk mag men pas spreken van een histiocyt als op basis
van immuun-histiochemische kleuringen dit bewezen wordt (4).
Hier wordt o.m. ACM1 voor gebruikt (4).
Histiocytoom:
(Goedaardige) neoplasia uitgaande van histiocyten (2).
Histiocytosis:
Vermeerdering van het aantal histiocyten in het bloed en beenmerg, lymfeklieren en in de weefsels (2).
1. Juncqueira
L.C. and Carneiro J. (1981) Basic Histology Lange Medical Publications
Los Altos. 3th edition.
2. Dorland's illustrated medical dictionary (1982) W.B. Saunders
Company Philadelphia 23th edition.
3. Okun M.R. and Edelstein L.M. (1976) Gross and Microscopic
Pathology of the Skin. Dermatopathology Foundation Press, Boston.
1st edition. pp 16-18
4. Magnol J.P. and Marchal Th. (1992) New classification of
Canine and Feline Cutaneous Histiocytic and Fibrohistiocytic
tumours, Proceedings Rome, pp 21-33
5. Muller G.H., Kirk R.W. and Scott D.W. (1989) Small Animal
Dermatology. 4th edition. W.B. Saunders Company

Histiocytoom (canine cutaneous histiocytoma):
Kliniek:
Een histiocytoom komt relatief vaak (50%) voor bij jonge honden (![]() 2 jr) maar zelden bij de kat (5). Ze groeien snel maar verdwijnen
eveneens snel. De predilectieplaats is meestal oren, hoofd en
de extremiteiten (1,4). Ze zijn meestal kleiner dan 1-2 centimeter.
Ze voelen stevig aan liggen los en verheven. De haargroei op
de tumor is gering. Ulceratie treedt soms (1) tot vaak op (5).
Het komt meer voor bij tekkels (1,5), boxers (1,4,5), Duitse
Doggen (4,5), Cocker Spaniels (5) en Shelties (5). Er is geen
sex-predispositie (5). Etiologisch wordt gedacht aan een virale
component (2,5).
2 jr) maar zelden bij de kat (5). Ze groeien snel maar verdwijnen
eveneens snel. De predilectieplaats is meestal oren, hoofd en
de extremiteiten (1,4). Ze zijn meestal kleiner dan 1-2 centimeter.
Ze voelen stevig aan liggen los en verheven. De haargroei op
de tumor is gering. Ulceratie treedt soms (1) tot vaak op (5).
Het komt meer voor bij tekkels (1,5), boxers (1,4,5), Duitse
Doggen (4,5), Cocker Spaniels (5) en Shelties (5). Er is geen
sex-predispositie (5). Etiologisch wordt gedacht aan een virale
component (2,5).
Histologie:
Ze worden gekenmerkt door een hoge mitoseindex (![]() 10) (1,4,5),
het zijn ovale cellen met een grote kern en overvloedig cytoplasma.
De tumor wordt gekarakteriseerd door het feit dat het een uniforme
laag van veelvormige histiocyten de dermis en subcutis infiltreren
en de collagene vezels en adnexa verdringen (5). D.m.v. cytochemische
kleuringstechnieken kan definitief gezegd worden dat het een
histiocyt is. De aanwezigheid van een reticulaire aggregatie
in het cytoplasma zou een aanduiding voor virale inductie zijn
(2). Lymphocytaire infiltratie en necrose kan het beeld in een
later stadium compliceren.
10) (1,4,5),
het zijn ovale cellen met een grote kern en overvloedig cytoplasma.
De tumor wordt gekarakteriseerd door het feit dat het een uniforme
laag van veelvormige histiocyten de dermis en subcutis infiltreren
en de collagene vezels en adnexa verdringen (5). D.m.v. cytochemische
kleuringstechnieken kan definitief gezegd worden dat het een
histiocyt is. De aanwezigheid van een reticulaire aggregatie
in het cytoplasma zou een aanduiding voor virale inductie zijn
(2). Lymphocytaire infiltratie en necrose kan het beeld in een
later stadium compliceren.
Therapie:
Metastasering
treedt niet op en vaak verdwijnen ze spontaan binnen 3 tot 6
maanden (1,5). Soms worden corticosteroiden erbij gegeven (0.5
- 1 mg/kg) (4) of vindt chirurgie/cryochirurgie plaats (5).
Discussie: Magnol (6) beschrijft vrij uitvoerig op basis waarvan hij en de zijne vindt dat gesproken moet worden van een canine cutaneous langerhans cell tumour. ACM1 een monoclonale specifiek antilichaam voor honden macrophagen (7) bleek ongevoelig voor eerder beschreven histiocytomen (8). Daarentegen waren ze wel positief voor CD1a (6) en de (mensen en knaagdieren) marker voor langerhans cellen. Dit onderzoek lijkt dus aan te tonen dat het dus een Langerhans cel is. Langerhans cellen en kernen zijn echter qua morfologie anders dan histiocyten.
1. Taylor D.O.N.,
Dorn C.R. and Luis O.H. (1969) Morphologic and biologic characteristics
of the canine histiocytoma Cancer Research 26 83-92
2. Glick A.D., Holscher M. and Campbell G.R. (1976) Canine
cutaneous histiocytoma, ultrastructural and cytochemical observations.
Veterinary Pathology 13, 13-17
3. Baker K.P., and Thomsett L.R. (1990) Canine and Feline Dermatology
Blackwell Scientific Publications. London. 1st edition. pp 186-187
4. Willemse T. (1991) Clinical dermatology of dogs and cats.
Wetenschappelijke uitgeverij Bunge. 1ste editie. pp 115-117
5. Muller G.H., Kirk R.W. and Scott D.W. (1989) Small Animal
Dermatology. 4th edition. W.B. Saunders Company
6. Magnol J.P. and Marchal Th. (1992) New classification of
Canine and Feline Cutaneous Histiocytic and Fibrohistiocytic
tumours, Proceedings Rome, pp 21-33
7. Marchal T., Caux C., Magnol J.P., Fournell C., Chabanne L.,
Rigal D., and Monier J.C. Identification of canine monocyte/macrophage
on paraffin sections by a new monoclonal antibody (ACM1) (submitted)
(referentie van 6)
8. Marchal T. (1989) thesis (referentie van 6)

Fibro-histiocytoom, fibreus histiocytoom of dermatofibroom:
Kliniek:
Het voorkomen is zelden, voor de hond, tot zeer zelden, voor de kat (2,3). De aandoening zou meer voorkomen bij Collies. Over het algemeen wordt de aandoening gezien bij honden van 2 tot 4 jaar oud zonder geslachtsvoorkeur. De cutane fibro-histiocytomen komen meestal multipel op het gezicht voor. Ze zijn stevig, duidelijk omlijnd. De epidermis kan hyperpigmentatie vertonen en een geringe mate van hyperkeratose vertonen (5).
Histologie:
Er is discussie over de origine van de cel (2,5). Hiermee wordt bedoeld dat de gedachte is dat een mesenchymale cel differentieert in de richting van histiocyten, fibroblasten of endotheliale cellen. Overheerst de fibroblastaire component is het een dermatofibroom of fibreus dermatofibroom. Wanneer histiocyten overheersen is het een histiocytoom of cellulaire dermatofibroom. Wanneer de endotheliale cel overheerst is het een scleroserend hemangioom. De tumor wordt in het algemeen zoals zij bekend is bij de hond gekenmerkt door weinig collageen vorming en een meerderheid van fibroblasten en histiocyten (1,2). De indeling bij histiocytomen berust op het onderzoek van Fitzpatrick (1987). Hierbij wordt met behulp van histiochemische technieken het bewijs geleverd. De tumor kan direct onder de epidermis liggen, dermaal liggen maar ook meer subcutaan liggen. De mitoseindex is laag.
Therapie:
Zowel chirurgie als sublesionale of systemische behandeling met corticosteroiden wordt gekozen (2). Over het algemeen is de behandeling met corticosteroiden effectief. In een aantal gevallen moest aan de therapie azothioprine (2 mg/kg om de dag) worden toegevoegd (4).
1. Smith J.S. (1976) Infiltrative corneal lesions resembling fibrous histiocytoma : Clinical and pathological findings in 6 dogs and 1 cat. Journal of the American Veterinary Medical Association 169, 722-734
2. Muller G.H., Kirk R.W. and Scott D.W. (1989) Small Animal Dermatology. 4th edition. W.B. Saunders Company
3. Fritzpatrick T.B. et al., (1987) Dermatology in General Medicine II. Mc Graw-Hill Book Company, New York.
4. Latimer C.A. (1983) Azothioprine in the manegment of fibrous histiocytoma in two dogs Journal of the American Animal Hospital Association 19,155
5. Okun M.R. and Edelstein L.M. (1976) Gross and Microscopic Pathology of the Skin. Dermatopathology Foundation Press, Boston. 1st edition. pp 780-785
6. Magnol J.P. and Marchal Th. (1992) New classification of Canine and Feline Cutaneous Histiocytic and Fibrohistiocytic tumours, Proceedings Rome, 21-33
Maligne fibro-histiocytomen, maligne fibreus histiocytoom (M.F.H.)
(voorheen fibrosarcoom):
Kliniek:
Ze komen zelden voor bij zowel de oudere hond als oudere kat (1,2). Bij de kat zou de tumor vaker dan bij de hond voorkomen (3). Er bestaat geen geslachts of rasvoorkeur. Ze komen meestal solitair voor. Ze zijn stevig, weinig begrensd, variabel in grootte en subepidermaal/subcutaan gelegen. Ulceratie is mogelijk. Predelectieplaatsen zouden de nek, ledematen en thorax zijn (1,3). Alhoewel de tumoren invasief groeien metastaseren ze zelden.
Histologie:
De oorsprong van de cel is waarschijnlijk mesenchymaal (1). Ze worden verder gekarakteriseerd als een infiltratief groeiende massa met overwegend veelvormige histiocyten, fibroblasten en meerkernige reuscellen. De mitoseindex is hoog. Een aantal eerder beschreven fibrosarcomen bleek later een maligne fibro histiocytoom te zijn (3). Er worden meerdere typen naar celtype en morfologie te onderscheiden, gezien (3). Magnol (3) beschrijft labeling met ACM1 en concludeert dus dat het histiocyten betreft.
Therapie:
Na chirurgie kan recidief optreden. Daar er slechts weinig beschreven zijn is er dus ook weinig over bekend.
1. Muller G.H., Kirk R.W. and Scott D.W. (1989) Small Animal Dermatology. 4th edition. W.B. Saunders Company
2. Renlund, R.C. and Prhzker K.P.H. (1984) Malignant fibrous histiocytoma involving the digit in a cat. Vet Pathology 21, 422
New classification of Canine and Feline Cutaneous Histiocytic and Fibrohistiocytic tumours, Proceedings Rome, pp 21-33
Cutane histiocytosis (voorheen maligne multicentrische histiocytosis):
Kliniek:
Cutane histiocytosis is een goedaardige histiocytaire proliferatieve aandoening. Er wordt vooralsnog geen leeftijds- (2 tot 13 jaar (5)), ras- of sex voorkeur gezien. De leasies komen multipel voor. Het uiterlijk is een erythemateuze dermale of subcutane plaque of nodulus (f 1 tot 5 cm) (3). Er is geen voorleukslokalisatie. De aandoening was eerder op basis van de klinische presentatie (multipele plaques/noduli) en het histologische patroon (infiltratief, hoge mitoseindex) beschreven als maligne multicentrische histiocytosis.
Histologie:
Het wordt gekarakteriseerd door een nodulaire tot diffuse dermale tot subcutane infiltratie met normale histiocyten. Zowel lymfocyten en neutrofielen polymorfkernige kunnen gezien worden.
Therapie:
De leasies kunnen verdwijnen en komen. Muller et al. (1989) melden nog dat een behandeling met hoge dosis van glucocorticosteroiden en cytostatica variabele resultaten geeft. Magnol (4) beschouwd deze aandoening echter als een immuun-gemedieerd proces geïnduceerd tengevolge van een onbekend agens. Zij (6) beschouwen het dan ook als een steriel granuloom/ pyogranuloom.
1. Thornton R.N. and Tisdall C.J. (1988) Multiple cutaneous histiocytosis in two dogs. New Zealand Veterinary Journal 36(4), 192-193
2. Mays, M.B.C. and Bergeron J.A. (1986) Cutaneous histiocytosis in dogs Journal of the American Veterinary Medical Association. 188, 377-380
3. Muller G.H., Kirk R.W. and Scott D.W. (1989) Small Animal Dermatology. 4th edition. W.B. Saunders Company
4. Magnol J.P. and Marchal Th. (1992) New classification of Canine and Feline Cutaneous Histiocytic and Fibrohistiocytic tumours, Proceedings Rome, pp 21-33
5. Calderwoods-Mays M.B., and Bergeron J.A. (1988) Cutaneous histiocytosis in dogs Journal of the American Veterinary Medical Association 188(4), 377-381
Maligne histiocytose:
Kliniek:
Het zijn zelden voorkomende maligne neoplasiën van histiocytaire oorsprong waarvan de oorzaak vooralsnog onbekend is (5). Maligne histiocytose komt voor bij diverse rassen zonder geslachtsvoorkeur. Meestal betreft het oudere dieren (5). De aandoening is ook beschreven bij voornamelijk mannelijke Berner Sennen Honden (1,2,5). Het klinisch beeld bevat depressie, anorexie, algehele malaise, gewichtsverlies en een lymphadenopathie. Een pancytopenie kan aanwezig zijn. Juist bij maligne histiocytosis zijn de longen aangedaan waar vanuit de ziekte begint (6). Als de huid in het proces betrokken is, wat slechts zelden het geval is, dat kunnen intradermale gelokaliseerde leasies van f 5 cm gezien worden.
Histologie:
Het wordt gekarakteriseerd door een nodulaire tot diffuse diepe dermale tot zelfs subcutane infiltratie (4). De infiltraten in de huid vertonen niet typische histiocyten. De cellen vertoonden phagocytose (4,5). Daarnaast viel op dat de cel grootte variabel was. De kernen waren onregelmatig vergroot met meerder kleine nucleoli. De mitoseindex was hoog i.t.t. systemische histiocytosis. Wellman et al., (1988) beschrijven een cellijn opgezet op basis van een canine maligne histiocytosis waarbij de diagnose door uitgebreid onderzoek werd (her-) bevestigd.
Therapie:
Het verloop is snel en de meeste patiënten sterven in korte tijd.
1. Magnol J.P. and Marchal Th. (1992) New classification of Canine and Feline Cutaneous Histiocytic and Fibrohistiocytic tumours, Proceedings Rome, pp 21-33
2. Tisdall C.J. and Thornton R.N. (1988) Malignant histiocytosis in a Bernese Moutain dog. New Zealand Veterinary Journal 36(1),43
3. Wellman M.L., Krakowka S., Jacobs R.M., Kociba G.J. (1988) A macrophage-monocyte- cell line from a dog with malignant histiocytosis. In Vitro Cellular and Development Biology 24(3), 223-229
4. Muller G.H., Kirk R.W. and Scott D.W. (1989) Small Animal Dermatology. 4th edition. W.B. Saunders Company
5. Moore P.F., and Rosin A. (1986) Malignant histiocytosis of Bernese Moutain Dogs. Vet. Pathol. 23, 1
6. Rosin A. Moore P., and Dubielzig R. (1986) Malignant histiocytosis in Bernese Moutain dogs. Journal of the American Veterinary Medical Association. 188(9), 1041-1045
Systemische histiocytose:
Kliniek:
Systemische histiocytose is een histiocytaire proliferatieve aandoening (2). Het voorkeursras lijkt de Berner Sennenhond te zijn. De aandoening kwam voornamelijk bij mannelijke dieren van 2 tot 8 jaar voor (3). Verder komt de ziekte bij diverse rassen ongeacht leeftijd of sexe, zelden, voor (1).
Gezien wordt door het gehele lichaam diffuse en/of nodulaire infiltraten in diverse organen. Met name bij systemische histiocytosis was bij alle Berner Sennenhonden de huid aangedaan (3). De huidafwijkingen beperkten zich tot multipele erythemateuze papels, plaque's, noduli, ulcera en een exsudatieve dermatitis (1,2,3,5,6). De leasies, met een voorkeurslokalisatie voor scrotum, oogleden en neus komen over het algemeen gegeneraliseerd/multifocaal voor.
Het klinisch beeld bestaat verder uit anorexie, gewichtsverlies en respiratoire bezwaren. De meeste patiënten vertoonden bij euthanasie histiocytaire infiltraten in de meeste organen zoals longen, lever, milt, been merg en lymfeknopen (1,3).
Histologie:
Deze wordt gekenmerkt door een oppervlakkige en diepe perivasculaire, nodulaire of juist diffuse infiltraten van normaal ogende histiocyten (1,2). De histiocytaire oorsprong is zowel op basis van morfologie, histio-enzymologisch onderzoek en immuun-histiochemisch onderzoek uitgevoerd (4).
Therapie:
Corticosteroiden en cytostatica hadden vooralsnog geen effect (1). Het verloop kan of snel en fataal zijn maar soms is het verloop ook fluctuerend met episodes van dragelijkheid maar ook duidelijke terugval. De overlevingstermijn is 2 tot 48 maanden (4).
1. Scott D.W., Angarano D.K. and Suter M.M. (1987) Systemic histiocytosis in two dogs. Canine practice 14(3), 7-9
2. Muller G.H., Kirk R.W. and Scott D.W. (1989) Small Animal Dermatology. 4th edition. W.B. Saunders Company
3. Moore P.F. (1984) Systemic histiocytosis of Bernese Mountain Dogs. Vet. Pathol. 21, 554
4. Magnol J.P. and Marchal Th. (1992) New classification of Canine and Feline Cutaneous Histiocytic and Fibrohistiocytic tumours, Proceedings Rome, 21-33
5. Bellstrom L. (1985) Systemisk histiocytos - forsta fallet i Sverige. Svensk Veterinatidning. 37, 678-680
Ocular manifestation of systemic histiocytosis in a dog. JAMVA 201(8),1229-1232
Overige literatuur inclusief abstracts:
(1) Penninck D, Smyers B, Webster CR, Rand W, Moore AS: Diagnostic value of ultrasonography in differentiating enteritis from intestinal neoplasia in dogs. Vet Radiol Ultrasound 2003; 44(5):570-575.
Abstract: One hundred and fifty dogs with histopathologically confirmed intestinal disease were evaluated retrospectively. Sixty-one dogs had enteritis and 89 dogs had intestinal neoplasia. Ultrasonographic findings including the thickness and distribution of the intestinal lesion, the integrity of intestinal wall layering, regional lymph node thickness, the location of the intestinal segment involved, and regional motility were evaluated. Dogs with intestinal tumor had wall thickness (1.5 cm) significantly greater than dogs with NSE lesions (0.6 cm; p ![]() 0.001). Ninety-nine percent of dogs with intestinal tumor had loss of wall layering while 88% of dogs with NSE had normal or altered wall layering (p
0.001). Ninety-nine percent of dogs with intestinal tumor had loss of wall layering while 88% of dogs with NSE had normal or altered wall layering (p ![]() 0.001). Dogs with NSE were significantly more likely to have diffuse lesion (72%) than dogs with intestinal tumor (2%; p
0.001). Dogs with NSE were significantly more likely to have diffuse lesion (72%) than dogs with intestinal tumor (2%; p ![]() 0.001). Lymph node median thickness in 24/61 dogs with NSE was 1.00 cm. The median thickness of the lymph nodes in 56/89 dogs with intestinal tumors was 1.9 cm. A multivariate analysis showed that loss of wall layering alone was an excellent predictive factor in differentiating intestinal tumor from NSE. In our population, dogs with loss of intestinal wall layering were 50.9 times more likely to have a tumor than enteritis
0.001). Lymph node median thickness in 24/61 dogs with NSE was 1.00 cm. The median thickness of the lymph nodes in 56/89 dogs with intestinal tumors was 1.9 cm. A multivariate analysis showed that loss of wall layering alone was an excellent predictive factor in differentiating intestinal tumor from NSE. In our population, dogs with loss of intestinal wall layering were 50.9 times more likely to have a tumor than enteritis
(2) Affolter VK, Moore PF: Localized and disseminated histiocytic sarcoma of dendritic cell origin in dogs. Vet Pathol 2002; 39(1):74-83.
Abstract: Canine histiocytic proliferative disorders include a wide spectrum of diseases characterized by different biologic behaviors. The etiology and pathogenesis of these diseases are largely unknown. The clinicopathologic, morphologic and immunophenotypic characteristics of canine localized and disseminated histiocytic sarcoma were examined in 39 dogs. Rottweilers, Bernese Mountain Dogs, and retrievers were most commonly affected (79%). Localized histiocytic sarcomas (19 dogs) arose from a single site, and metastatic lesions were observed in draining lymph nodes. Predilection sites were subcutis and underlying tissues on extremities, but tumors occurred in other locations, including spleen, lung, brain, nasal cavity, and bone marrow. Disseminated histiocytic sarcomas (20 dogs), a multisystem disease previously described as malignant histiocytosis, primarily affected spleen, lungs, bone marrow, liver, and lymph nodes. Both localized and disseminated canine histiocytic sarcomas were composed of pleomorphic tumor cell populations. CD1+, CD4-, CD11c+, CD11d-, MHC II+, ICAM-1 +, Thy-1 +/- tumor cells were identified in all snap-frozen samples (31 dogs). This phenotype is characteristic for myeloid dendritic antigen-presenting cell lineage. Hence, canine localized and disseminated histiocytic sarcomas are likely myeloid dendritic cell sarcomas. Dendritic antigen-presenting cells are a heterogeneous cell population with regards to their ontogeny, phenotype, function, and localization. The exact sublineage of the proliferating dendritic antigen-presenting cells involved in canine histiocytic sarcomas remains to be determined. Phenotypic analysis of formalin-fixed tissues from eight dogs was limited by available markers. Morphologic features and the phenotype CD18+, CD3-, and CD79a- were the most useful criteria to indicate likely histiocytic origin
(3) Ramirez S, Douglass JP, Robertson ID: Ultrasonographic features of canine abdominal malignant histiocytosis. Vet Radiol Ultrasound 2002; 43(2):167-170.
Abstract: Ultrasonographic features of canine abdominal malignant histiocytosis (MH) of 16 dogs are reported. The most common finding was the presence of hypoechoic nodules in the spleen, some of which caused distortion of the splenic margin. The liver was the second-most commonly affected organ. Hepatic ultrasonographic features were highly variable, including hypoechoic, hyperechoic, or mixed echogenic lesions. Other common ultrasonographic abnormalities included hypoechoic nodules in the kidneys and mesenteric and medial iliac lymphadenopathy. The results of this study suggest that the ultrasonographic appearance of canine abdominal MH is nonspecific, and definitive diagnosis requires cytologic or histologic examination
(4) Chandra AM, Ginn PE: Primary malignant histiocytosis of the brain in a dog. J Comp Pathol 1999; 121(1):77-82.
Abstract: Malignant histiocytosis is a well-recognized canine tumour, occurring primarily in Bernese mountain dogs and characterized by disseminated histiocytic infiltration of multiple visceral organs. This report describes the light microscopical and ultrastructural features of a neoplasm composed of malignant histiocytes and confined to the brain. A poorly demarcated mass in the right parieto-occipital lobe of a miniature schnauzer was composed of loosely aggregated, pleomorphic cells with abundant eosinophilic cytoplasm, expanding the meninges. Many binucleated and multinucleated giant cells and mitotic figures were seen. Immunohistochemically, the tumour cells reacted intensely for lysozyme. Ultrastructurally, the neoplastic cells had features of histiocytic cells with abundant lysosomes. The findings in this case were strikingly similar to those of disseminated malignant histiocytosis described in other dog breeds
(5) Spangler WL, Kass PH: Splenic myeloid metaplasia, histiocytosis, and hypersplenism in the dog (65 cases). Vet Pathol 1999; 36(6):583-593.
Abstract: Splenectomy specimens from 65 dogs with severe, diffuse, sustained, and progressive splenomegaly were examined. The clinical signs, hematology, and serum chemistry values in for the dogs were not useful diagnostic features. Microscopic changes in the spleens were distinctive and consisted of 1) myeloid metaplasia, 2) histiocytosis, 3) erythrophagocytosis, and 4) thrombosis with segmental infarction. Ultrastructural features suggested proliferative changes in the splenic reticular cells and macrophages (reticular meshwork) that described a continuum from reactive changes associated with immunologic damage of erythrocytes to neoplastic proliferation of histiocytic components. Thirty percent of the dogs survived 12 months. Approximately one half (53%) of the dogs with complete postmortem evaluations showed multiorgan involvement with a tissue distribution and cell morphology consistent with histiocytic neoplasia. For the remaining dogs (47%), only splenic pathology was consistently present, and a specific cause of death was often not evident. Distinctive histologic changes in the splenic tissues-including mitotic activity, erythrophagocytosis, giant cell formation, thrombosis/ infarction, and the proportion and distribution of histiocytic and hematopoietic cells-were statistically evaluated for prognostic relevance. The presence of giant cells was the only reliable prognostic feature, and that was indicative of a fatal outcome. These descriptive changes of myeloid metaplasia in the canine spleen are compared with the human clinical and pathologic syndromes of 1) agnogenic myeloid metaplasia, 2) hemophagocytic syndromes, and 3) hypersplenism. These diseases in humans produce histopathologic changes in the spleen that are similar to those observed in the canine splenic tissue we examined in this study
(6) Uehlinger P, Glaus T, Hauser B, Reusch C: [Differential diagnosis of hypercalcemia--a retrospective study of 46 dogs]. Schweiz Arch Tierheilkd 1998; 140(5):188-197.
Abstract: The case records of 46 dogs with hypercalcemia were studied retrospectively. The most common cause of hypercalcemia was malignancy, of which the majority were diagnosed as having lymphosarcoma (LSA, n = 23). Interestingly only 15 had palpable lymphadenopathy. Other neoplasia were apocrine adenocarcinoma of the anal sac (n = 4), mammary adenocarcinoma (n = 2), anaplastic carcinoma (n = 1), and malignant histiocytosis (n = 1). Non-neoplastic reasons for hypercalcemia were hypoadrenocorticism (n = 5), acute renal failure (n = 2), chronic renal failure (n = 2), hypervitaminosis D (n = 1), and primary hyperparathyroidism (n = 1). In 4 cases no definitive diagnosis could be obtained. Moderate to marked hyperphosphatemia and azotemia was found in all dogs with primary renal failure and in 4 of 5 dogs with hypoadrenocorticism. In contrast only 4 of 31 dogs with neoplasia showed (mild) hyperphosphatemia and 20 showed mild to moderate azotemia. Elevated PTH levels were found in dogs with primary chronic renal failure and with primary hyperparathyroidism, but also in one dog with neoplasia. Low PTH concentrations were measured in the dog with hypervitaminosis D and in 8 cases with neoplasia. Additional three cases with neoplasia had values in the reference range. CONCLUSIONS: 1. The most common cause of hypercalcemia is LSA. Absence of palpable lymphadenopathy does not exclude LSA and further diagnostic steps may be necessary 2. The combination of moderate to marked hyperphosphatemia suggests primary renal failure or hypoadrenocorticism. 3. An elevated PTH level is consistent with primary hyperparathyroidism, but does not exclude other causes of hypercalcemia
(7) Carioto L: Malignant histiocytosis in a Bernese mountain dog presenting as a mandibular mass. Can Vet J 1997; 38(2):105-107.
Abstract: A Bernese mountain dog was evaluated because of a gingival mass, multiple abdominal masses, and a pulmonary mass. Malignant histiocytosis was diagnosed based on cytological examination of splenic and bone marrow aspirates and histological examination of a bone marrow biopsy and the gingival mass. The case demonstrates that malignant histiocytosis is difficult to diagnose due to the variety of histiocytic disorders
(8) Ramsey IK, McKay JS, Rudorf H, Dobson JM: Malignant histiocytosis in three Bernese mountain dogs. Vet Rec 1996; 138(18):440-444.
Abstract: Malignant histiocytosis is a rare disease which is characterised by the neoplastic proliferation of tissue macrophages (histiocytes) leading to excessive phagocytosis of erythrocytes. The clinical signs and pathological findings in three Bernese mountain dogs are described. Two of the dogs had the same sire. The disease has been established as a familial problem in Bernese mountain dogs in other countries, although it has not been previously recorded in the United Kingdom
(9) Padgett GA, Madewell BR, Keller ET, Jodar L, Packard M: Inheritance of histiocytosis in Bernese mountain dogs. J Small Anim Pract 1995; 36(3):93-98.
Abstract: One hundred and twenty-seven cases of histiocytosis in Bernese mountain dogs (BMD) were evaluated to determine if the tumour is inherited. Family data ruled out autosomal recessive, autosomal dominant and sex-linked modes of inheritance. The trait was determined to be inherited with a polygenic mode of inheritance. The salient points permitting this conclusion are: pedigrees developed from independently selected propositi link up allowing the tracing of all cases through several generations; multiple cases occur in the same litter; multiple cases have been produced by given dams and sires; there is a higher frequency of the disease among offspring of affected parents when compared to offspring of normal parents that produced histiocytosis and all offspring in the general population of BMDs; the fact that histiocytosis is common in BMDs and rare in eight other breeds and accounts for 25.4 per cent of the 500 tumours studied in this breed. The heritability of this trait was calculated to be 0.298
(10) Paterson S, Boydell P, Pike R: Systemic histiocytosis in the Bernese mountain dog. J Small Anim Pract 1995; 36(5):233-236.
Abstract: Systemic histiocytosis is a rare familial histiocytic disorder seen in the Bernese mountain dog. This article documents six confirmed cases of the disease seen at the Animal Medical Centre between June 1992 and June 1994 and describes the different presentations of the disease, response to therapy and progression. Three of the dogs are still alive; of these, two are in remission six and 18 months later and in one case the owner refused treatment. Three of the cases were euthanased for humane reasons
(11) Brown DE, Thrall MA, Getzy DM, Weiser MG, Ogilvie GK: Cytology of canine malignant histiocytosis. Vet Clin Pathol 1994; 23(4):118-123.
Abstract: Cytologic features of bone marrow, tissue, and abdominal fluid in seven cases of malignant histiocytosis in dogs are described, and histopathology, hematology, and serum biochemistry of the cases are reviewed. Diagnosis of malignant histiocytosis was confirmed by tissue morphology and immunohistochemistry; neoplastic cells in all cases had positive immunoreactivity to lysozyme. This stain can be used to definitively establish the diagnosis of malignant histiocytosis on cytology specimens as well as tissue sections. Cytologic findings included numerous pleomorphic, large, discrete mononuclear cells with abundant, lightly basophilic, vacuolated, granular cytoplasm. Nuclei were round to oval to reniform with marked anisocytosis and anisokaryosis; nucleoli were prominent. Mitotic figures, often bizarre, were occasionally seen. Multinucleated giant cells and phagocytosis of erythrocytes and leukocytes were prominent features in cytologic preparations in four cases. Four dogs were anemic, five dogs were thrombocytopenic, and three dogs were hypercalcemic. Breeds affected included Doberman Pinscher (1), Golden Retriever (2), Flat Coated Retriever (3), and mixed-breed dog (1)
(12) Hayden DW, Waters DJ, Burke BA, Manivel JC: Disseminated malignant histiocytosis in a golden retriever: clinicopathologic, ultrastructural, and immunohistochemical findings. Vet Pathol 1993; 30(3):256-264.
Abstract: Diagnosis of malignant histiocytosis (MH), a disorder characterized by systemic proliferation of morphologically atypical histiocytes and their precursors, in an 8-year-old neutered female Golden Retriever was based on light and electron microscopic and immunohistochemical findings. Clinically, the dog presented with unilateral forelimb lameness. Eight days after surgical exploration of a swollen brachium, the dog developed sudden onset of posterior paresis, fecal and urinary incontinence, and a flaccid tail. Necropsy revealed infiltrative and nodular lesions in the right forelimb and regional lymph nodes, thoracic and abdominal cavities, and lumbar epidural space. Gross lesions were not found in the lungs or integument. Histopathologic examination showed infiltrates of atypical histiocytes in skeletal muscle, joint, and regional lymph nodes of the right forelimb; intercostal muscle; lung; liver; spleen; pancreas; kidneys; and spinal dura. Most tumor infiltrates were nodular and composed of loosely aggregated cells that were 10-30 microns in diameter with abundant eosinophilic to foamy cytoplasm, had central or eccentric nuclei, and were periodic acid-Schiff negative. Many binucleated cells, multinucleated giant cells, and mitotic figures were seen. Tumor cells contained phagocytosed erythrocytes, mononuclear cells, and some leukocytes. Ultrastructural features of tumor cells included cytoplasmic lipid droplets, lysosomes, and phagolysosomes. Immunohistochemical studies on paraffin-embedded sections showed positive reactivity to human T-cell Ag (clone UCHL-1) and for lysozyme, alpha-1-antitrypsin, and cathespin B. Polyclonal intracellular immunoglobulin reactivity and lectin binding (peanut, soybean, and wheat germ agglutinins and concanavalin A) were also demonstrated. Criteria for diagnosis of malignant histiocytic tumors and differential diagnosis are discussed
(13) Schmidt ML, Rutteman GR, van Niel MH, Wolvekamp PT: Clinical and radiographic manifestations of canine malignant histiocytosis. Vet Q 1993; 15(3):117-120.
Abstract: The results of clinical and radiographic examinations of 15 dogs with confirmed malignant histiocytosis (MH) were reviewed. The most common clinical signs were anorexia (14 dogs), weight loss (13 dogs), lethargy (13 dogs), anaemia (11 dogs), and dyspnoea and/or coughing (8 dogs). Radiographs revealed abnormalities in all dogs, either intrathoracic (pulmonary nodules or consolidation [7 dogs], mediastinal masses [10 dogs], and incidentally pleural effusion [3 dogs]) or abdominal (hepatomegaly [6 dogs] and splenomegaly [2 dogs]), or both. MH occurs relatively frequently in Bernese Mountain dogs. Both clinical and radiographic signs are non-specific, but when they are present in a middle-aged Bernese Mountain dog, MH should be included in the differential diagnosis
(14) Mays MB, Bergeron JA: Cutaneous histiocytosis in dogs. J Am Vet Med Assoc 1986; 188(4):377-381.
Abstract: Multifocal cutaneous histiocytic lesions were recognized in 9 dogs. Clinically, the dogs had multiple erythematous plaques or nodules in the skin (1 to 5 cm diameter). Histologically, the lesions were comprised of dermal or pannicular infiltrates of large histiocytic cells, with varying numbers of other inflammatory cells intermixed. By electron microscopy, the cells resembled those of canine cutaneous histiocytoma. The lesions seemed to wax and wane and appeared in new sites, regardless of treatment. The dogs ranged in age from 2 to 13 years; 7 dogs were under 6 years of age. Both sexes and various breeds were represented. An infectious agent could not be identified
(15) Moore PF, Rosin A: Malignant histiocytosis of Bernese mountain dogs. Vet Pathol 1986; 23(1):1-10.
Abstract: A second histiocytic proliferative disorder, which resembled malignant histiocytosis of man, was identified in 13 Bernese mountain dogs. Malignant histiocytosis was clearly distinct from systemic histiocytosis, which was reported earlier in this breed. Eleven cases involved male dogs. Ten dogs occurred in the same family line as the dogs afflicted with systemic histiocytosis. Clinical or radiological evidence of pulmonary involvement was present in nine dogs. Neurological disturbances were present in five dogs. Anemia was observed in five dogs and was associated with prominent erythrophagocytosis in two instances. The clinical course was rapidly progressive. Necropsy examinations revealed that infiltrates were especially frequent in the lungs and hilar lymph nodes. Other lymph nodes, liver, spleen, and central nervous system were also frequently involved. Evidence for primary pulmonary involvement was present in seven dogs. The original diagnosis in seven cases was large cell anaplastic carcinoma of the lung by light microscopy only. The infiltrates were composed of large, pleomorphic, phagocytic mononuclear cells and multinucleated giant cells which also manifested marked cytological atypia and numerous, frequently bizarre, mitotic figures. Ultrastructural studies and the immunohistochemical demonstration of lysozyme and alpha 1-antitrypsin in the tumor cells in the majority of cases were consistent with a macrophage origin
(16) Rosin A, Moore P, Dubielzig R: Malignant histiocytosis in Bernese Mountain dogs. J Am Vet Med Assoc 1986; 188(9):1041-1045.
Abstract: Malignant histiocytosis was diagnosed in 10 male and 1 female Bernese Mountain Dogs. Nine of these dogs were closely related. The disease was characterized by a rapidly progressive and inevitably fatal course. Clinical signs varied, but lethargy, anorexia, weight loss, and respiratory and CNS abnormalities predominated. The lungs were the primary site of tumor involvement in 10 dogs. The eleventh dog had lymphadenopathy and severe anemia. Metastatic lesions were detected in all dogs. Anaplastic pulmonary carcinoma was diagnosed originally in 6 of the 11 cases, but this diagnosis was changed to malignant histiocytosis after electron microscopic examination of tissues and immunohistochemical identification of histiocytic markers in the tumor cells
(17) Wellman ML, Davenport DJ, Morton D, Jacobs RM: Malignant histiocytosis in four dogs. J Am Vet Med Assoc 1985; 187(9):919-921.
Abstract: The clinical and pathologic features of 4 dogs with malignant histiocytosis were evaluated. The most common clinical signs were weight loss, lethargy, lymphadenopathy, hepatosplenomegaly, and anemia. Neoplastic histiocytic infiltrates most commonly were found in the spleen, bone marrow, liver, or lymph nodes. Malignant histiocytosis was considered as a differential diagnosis for anemic dogs with lymphadenopathy and/or hepatosplenomegaly
(18) Moore PF: Systemic histiocytosis of Bernese mountain dogs. Vet Pathol 1984; 21(6):554-563.
Abstract: A histiocytic proliferative disorder was identified in six closely related Bernese mountain dogs. Clinical signs included anorexia, weight loss, stertorous respiration, and conjunctivitis with marked chemosis. Multiple cutaneous nodules were distributed over the entire body but were especially prevalent in the scrotum, nasal apex, nasal planum, and eyelids. Lesions consisted of perivascular infiltrates of large histiocytes as well as minor populations of lymphocytes, neutrophils, and eosinophils. Histiocytes were further characterized by enzyme histochemistry and electron microscopy. Necropsy examinations of four dogs revealed that the histiocytic infiltrates were widespread and involved skin, lung, liver, bone marrow, spleen, lymph nodes, kidneys, testes, orbital tissues, and others. However, skin and peripheral lymph nodes were more consistently involved. The disease course was punctuated by remissions and relapses not clearly influenced by conventional therapeutic measures. Preliminary results of an experimental therapeutic regimen involving administration of bovine thymic extracts in two dogs are present. The relationship of the disorder to other human and canine histiocytic proliferative disorders is discussed
Dr. Paul J.J. Mandigers
Dierenarts-specialist Interne Geneeskunde

Veterinair
Specialistisch Centrum "De Wagenrenk"
Keijenbergseweg 18
6705 BN Wageningen

